BCS implants are a single-piece immediate-loading dental implant system manufactured by Ihde Dental. They belong to the Strategic Implant concept and are designed primarily for cortical anchorage in the upper and lower jaw.
Unlike conventional two-stage implants, BCS implants are not selected only according to the height and volume of cancellous bone. Their main purpose is to achieve mechanical stability by engaging stable cortical bone. This makes them particularly useful in cases where the available bone is reduced, uneven, or unsuitable for conventional implant placement without additional grafting.
BCS implants are commonly used in immediate loading protocols, especially for segmental bridges and full-arch circular bridges. In suitable clinical situations, they may also be placed immediately after extraction, provided that sufficient basal support is available.
The BCS Implant Series
The BCS series includes several implant diameters, lengths and prosthetic head designs. The range includes small abutment head implants, large abutment head implants and BCS MU implants for screw-retained multi-unit prosthetics.
The implants are made from a strong biocompatible titanium alloy, Ti6Al4V. They have a mechanically smoothed surface and a self-tapping thread with anti-rotation protection. The anti-rotation design helps protect the implant from unintended unscrewing before the prosthesis is fitted.
The smaller 2.7 mm and 3.0 mm implants are generally considered supporting or additional implants. They are used to increase the stability of the implant-prosthetic construction and to help create three-point cortical support. They are not normally intended as single-tooth implants on their own.
The wider BCS implants, including 4.6 mm, 5.5 mm, 7.0 mm, 9.0 mm, 10.5 mm and 12.0 mm versions, are used where wider cortical or basal support is available and where stronger prosthetic support is required.
Anatomical Location for BCS Implants
BCS implants are used in both the upper and lower jaw. Their main clinical role is to provide anchorage in cortical bone rather than relying only on soft cancellous bone.
Typical areas of use include:
- Posterior maxilla
- Anterior maxilla
- Posterior mandible
- Anterior mandible
- Extraction sockets, when basal support is sufficient
- Tubero-pterygoid region
- Cortical bone zones used for strategic implant anchorage
- Full-arch immediate-loading cases
- Segmental bridge restorations
In the upper jaw, BCS implants may be used where conventional implant placement is difficult because of limited vertical bone height, reduced bone volume, or sinus proximity. In these cases, the implant may be directed toward available cortical support rather than relying only on the alveolar ridge.
In the lower jaw, BCS implants may be used to engage stable cortical structures and provide rigid support for immediate splinting.
Bone Conditions for BCS Implants
BCS implants are especially relevant when the treatment plan requires anchorage in hard cortical bone.
They may be considered in situations such as:
- Reduced alveolar bone volume
- Thin ridges
- Post-extraction sites with sufficient basal support
- Atrophic jaw conditions
- Posterior maxilla with limited cancellous bone
- Cases where cortical bone remains available despite alveolar bone loss
- Full-arch rehabilitation where multiple implants can be splinted immediately
The important principle is not simply “how much bone is present,” but whether the implant can be anchored in stable cortical bone. This is why BCS implants are often discussed in relation to basal implantology and strategic implantology.
The 2.7 mm and 3.0 mm BCS implants are particularly useful in thin jaw areas as additional implants. When only these narrow implants are used in a very thin jaw, the manufacturer’s catalogue indicates that a larger number of implants may be required to create a stable implant-prosthetic system.
Anchorage Strategy
The anchorage strategy of BCS implants is cortical anchorage.
In practical terms, this means that the implant is inserted so that its thread engages one or more dense cortical bone layers. The goal is to create immediate mechanical stability, allowing the implants to be splinted with a prosthetic structure early in the treatment sequence.
The BCS system is described for anchorage in the 1st, 2nd and, where necessary, 3rd cortical. This is central to the Strategic Implant concept.
The anchorage strategy may include:
- Engagement of the crestal cortical bone
- Engagement of deeper basal cortical bone
- Bicortical or multicortical support where anatomy allows
- Tubero-pterygoid cortical anchorage in the posterior maxilla
- Strategic distribution of implants to support immediate splinting
- Three-point support in bridge and full-arch restorations
The implant-prosthetic system is designed to work as a splinted unit. For that reason, BCS implants are often used in segmental bridges or circular full-arch bridges rather than as isolated implants.
Immediate Loading Protocol
BCS implants are designed for immediate loading when the clinical conditions are suitable.
The manufacturer’s catalogue states that BCS implants are typically used for segments and circular bridges in an immediate splinting protocol. It also states that the prosthesis should be inserted before the 3rd post-operative day.
In clinical terms, this means that BCS implants are not usually left unloaded for several months in the same way as many conventional two-stage implant systems. Instead, the treatment concept depends on achieving strong mechanical anchorage at placement, followed by early prosthetic splinting.
The immediate loading protocol generally depends on:
- Adequate primary stability
- Correct implant distribution
- Sufficient cortical anchorage
- Rigid prosthetic splinting
- Controlled occlusion
- Appropriate case selection
- Surgical and prosthetic experience with strategic implantology
The prosthesis may be a segmental bridge or a full-arch circular bridge, depending on the case.
Clinical Case Study: How Dr Genchev Used BCS Implants in Severe Posterior Maxillary Atrophy
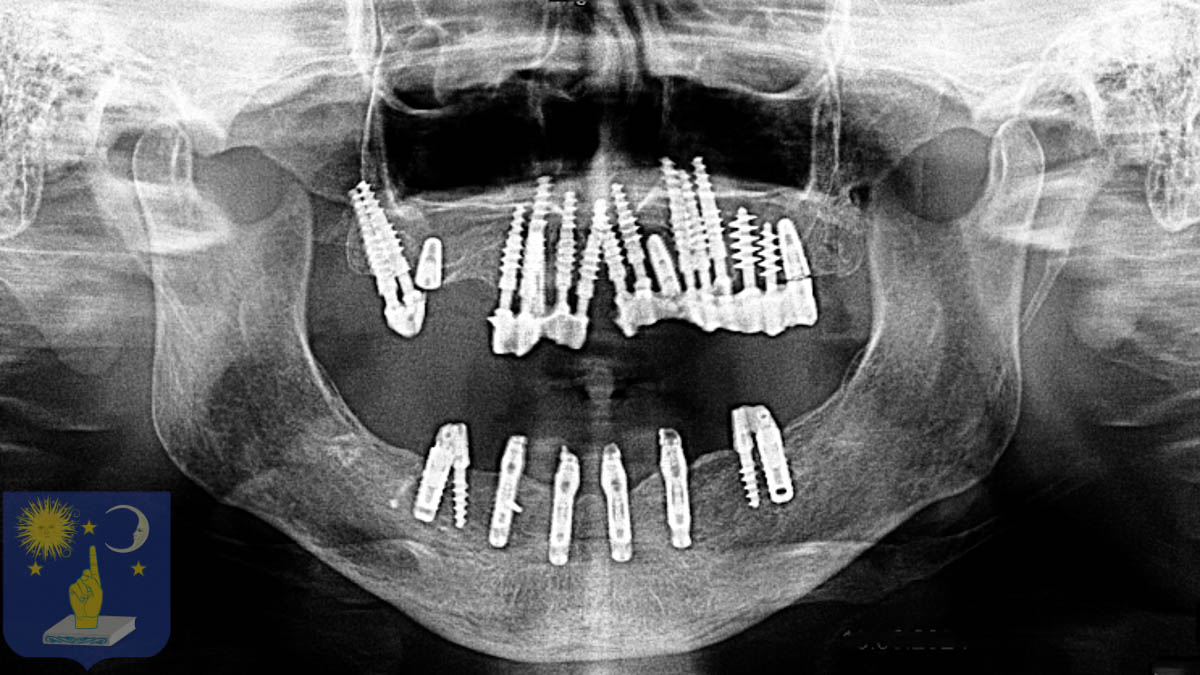
In Marie’s full-mouth rehabilitation, Dr Genchev used BCS implants in the right posterior maxilla, where the bone conditions were particularly demanding. This area showed severe resorption: the cancellous bone had disappeared, leaving mainly hard cortical bone.
For this reason, Dr Genchev selected the Ihde Dental BCS system. In this zone, the treatment goal was not cancellous bone compression, but pure cortical fixation. BCS implants were chosen because they are designed to anchor into dense cortical structures and provide immediate mechanical stability. Dr Genchev placed four BCS implants in the right posterior maxilla.
Case Studies For BCS Ihde Dental Implants
-
Basal Implants for Gum Disease
Dr. Genchev placed 25 basal dental implants, two permanent metal-ceramic bridges, and recreated Marc’s smile when he was a younger man, in one single 5-day visit in Plovdiv Bulgaria.
-
Dr Genchev Lower Jaw Restoration
Dr. Genchev transformed Aline’s life in just 5 days with basal implants, completing the lower jaw restoration that another basal implant dentist had declared too difficult.

-
Failed All-on-6 Saved with Basal Implants
Dr Genchev saved Françoise after she suffered a failed All-on-6 procedure. Full dental restoration with basal dental implants in 5 days treating prognathism for €9,990.
-
Dr Genchev Bone Atrophy Treatment with Basal Implants
Dr Genchev in Bulgaria successfully rehabilitates with basal implants Paul’s maxillary who suffered from severe bone atrophy and had experienced 3 failed bone grafts. Full dental restoration in 5 days for €6,500. Real case study showing why basal implants succeed where conventional implants fail.

-
Dr Genchev Dental Restoration for Gum Disease
Dr. Genchev transformed Véronique’s life in just 5 days with basal implants, restoring her ability to eat without pain and giving her back a confident smile.

-
Dental restoration for missing teeth and bone atrophy with basal implants
Dr Genchev completed the full mouth dental restoration for this patient who suffered from edentulism with severe bone atrophy in 1 visit of 5 days. The price for the full dental restoration was 8990 Euro.
