the Nasal Floor Cortex
The nasal floor cortex is the bony floor of the nasal cavity. The nasal floor cortex (Latin: pars nasalis ossis frontalis, or more precisely the cortex of the pars nasalis ossis maxillae) is the thin but dense bony plate that forms the lower boundary of the nasal cavity. It runs horizontally above the anterior maxillary dentition.
In the context of dental implantation, it is a dense cortical bone layer that sits immediately above the apices of the upper incisor and canine teeth. For implant planning in the anterior maxilla, it can serve as a valuable secondary cortical anchorage point that improves primary stability when the alveolar ridge is narrow or the cancellous bone is soft. It is one of the structures that makes Full Dental restoration of the upper jaw possible without bone grafting.
Key anatomical points:
- Location: Superior to the apices of the upper incisors and canines, forming the floor of the nasal cavity where it overlies the anterior maxillary alveolar process.
- Synonyms and alternative names: Nasal floor cortex, nasal cortex, cortical bone of the nasal floor, nasal cortical plate, floor of the nasal fossa.
- Adjacent structures: The nasal cavity superiorly, the maxillary alveolar process inferiorly, and the anterior nasal spine (Latin: spina nasalis anterior) at the midline.
- Bone characteristics: Thin but densely cortical. The nasal floor cortex is significantly more mineralized than the cancellous bone of the anterior maxillary alveolar process beneath it.
In a healthy dentition with no bone loss, the nasal floor is typically 2 to 3 mm above the root apices of the upper central incisors. In edentulous patients or patients with bone resorption, the distance between the alveolar crest and the nasal floor may be reduced, bringing the cortical nasal floor closer to the surface and making it more accessible as an anchorage target for implants.
Bone Quality of the Nasal Floor Cortex
Is the nasal floor cortex reliable enough for implant anchorage?
The nasal floor cortex is one of the denser cortical structures in the anterior maxilla. This is an important distinction because the anterior maxillary alveolar process typically contains D3 bone: a thin cortical layer with fine trabecular bone underneath. D3 bone can support implants.
The trabecular bone in the anterior maxilla compresses under implant insertion, which is how compression-type implants achieve primary stability there. But this cancellous bone is finer and less dense than mandibular trabecular bone, and when bone width is limited, as it often is in the anterior maxilla of edentulous patients, the compressive force alone may not produce enough stability for immediate loading.
The nasal floor cortex provides the solution. As a denser cortical structure, it acts as a second fixation point when the implant tip is long enough and correctly angled to reach it. The implant body compresses the cancellous bone in the alveolar process. The implant tip engages the cortical nasal floor above. The result is a combination of cancellous compression and cortical anchorage in a single implant, which significantly increases primary stability.
In terms of bone type, the nasal floor cortex behaves closer to D1 or D2 bone than the surrounding anterior maxillary alveolar bone.
Nasal Floor Cortex in Strategic Implantation
Why would my dentist aim for the nasal floor when placing implants in my front upper teeth?
The anterior maxilla is one of the most anatomically challenging zones for implant placement. Several factors combine to make it difficult:
- Bone is typically D3: thinner cortical shell, softer trabecular core.
- After tooth loss, the alveolar ridge loses width, often becoming very narrow buccolingually.
- The nasal cavity limits how far implants can go superiorly without entering the airway.
- Adequate primary stability is essential for immediate loading protocols.
In a narrow anterior alveolar ridge with soft D3 bone, an implant placed purely in cancellous bone may achieve borderline primary stability at best. This can be sufficient in delayed loading protocols but is not always adequate for an immediate-loading Full Dental bridge.
Engaging the nasal floor cortex changes this equation. By selecting the right implant length and using a slight palatal inclination, the implantologist can direct the implant tip to contact the dense nasal cortical bone. This adds a second point of mechanical fixation. The overall primary stability of the implant improves substantially.
This also means that the anterior maxilla can often be treated without bone grafting, even when the ridge is narrow. The nasal floor cortex compensates for what the cancellous bone alone cannot provide.
Planning this correctly requires:
- CBCT analysis to measure the height of the alveolar process, the position of the nasal floor and the available bone width.
- Implant length selection that allows the tip to reach the nasal cortex safely without perforating beyond it.
- Palatal inclination to direct the implant tip toward the cortical target while preserving the buccal bone and soft tissue.
Implant Selection for Nasal Floor Cortex Anchorage
Which implants are best suited to reach and engage the nasal floor cortex?
The right implant must be long enough to reach the nasal floor cortex, narrow enough to fit in a reduced alveolar ridge, and designed to achieve compression of the cancellous bone in the osteotomy path before its tip contacts the cortical structure.
Ihde Dental KOS Root is the most directly documented implant for nasal floor cortex anchorage in the case studies associated with this website. KOS Root is a compression screw implant. Its rough surface compresses the cancellous bone during insertion and the tip can engage the cortical nasal floor when the correct length and inclination are used. Its narrow diameters, particularly 3.0 mm and 3.5 mm, are well suited to the limited bone width of the anterior maxillary ridge.
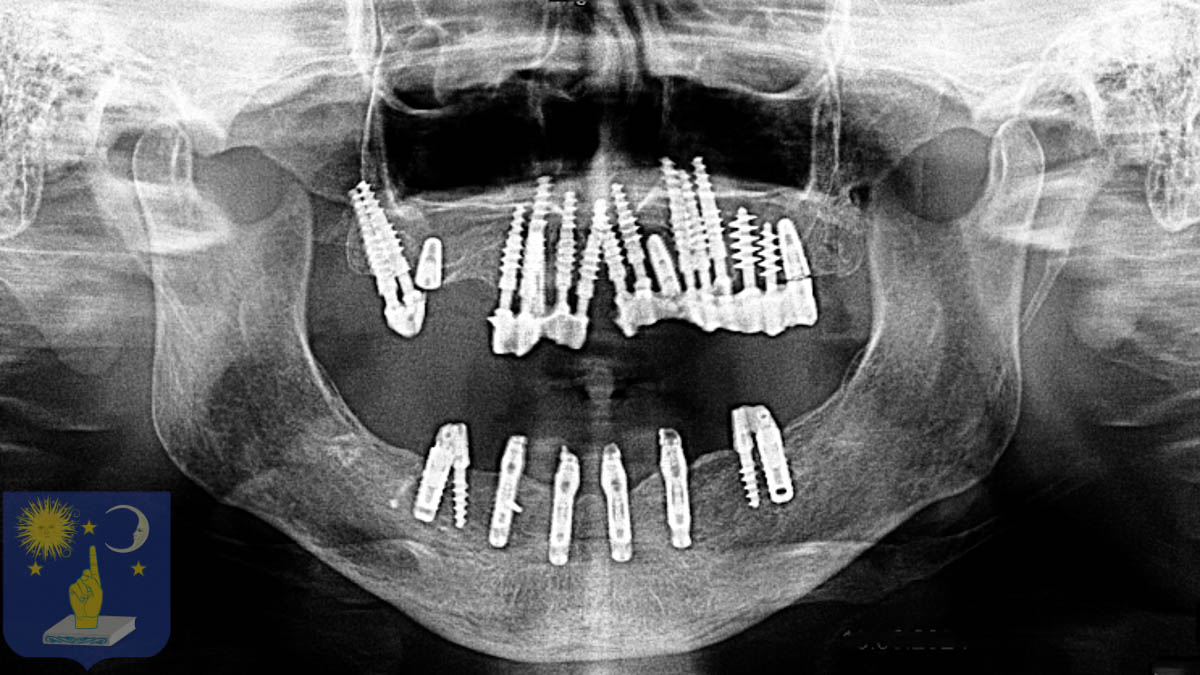
In Dr Genchev’s full restoration case, seven KOS Root implants at 3.5 x 16 mm were placed across positions 14 to 23 in the anterior maxilla. Each was inserted with slight palatal inclination. Each compressed the cancellous bone in the alveolar process and fixed its tip into the cortical bone of the nasal floor. This two-point anchorage strategy across the full anterior arch provided the primary stability needed for immediate loading.
In Dr Genchev’s gum disease case, TPG Uno implants were selected for the anterior maxilla and upper jaw. The TPG Uno was used to benefit from both the cancellous bone and the cortical bone of the nasal cortex to achieve primary stability, demonstrating that different implant systems can be matched to nasal floor anchorage depending on the bone conditions.
Ihde Dental TPG Uno is relevant in the anterior maxilla when both cancellous and cortical bone are present and the nasal floor is accessible. Its triple-thread design compresses cancellous bone and can engage cortical structures at the tip.
BasalFix Compressive-Fix is specifically noted for use in the anterior to mid-maxilla zone where the nasal floor cortex is reachable. The hybrid design compresses the cancellous bone body and engages the cortical tip, mapping directly onto the nasal floor anchorage strategy. Palatal inclination allows the tip to reach the nasal floor cortex.
BasalFix Basal, the cortical anchorage implant in the BasalFix range, lists the nasal floor cortex and palatal cortex as cortical targets in the mid-maxilla zone. At 3.5 x 12 to 16 mm with palatal inclination, it can achieve dual cortical fixation engaging both the alveolar cortex and the nasal floor.
Monoimplant Rough is designed for softer D3 and D4 bone. In the anterior maxilla, its rough calcium phosphate treated surface supports osseointegration in the softer alveolar bone, and the implant length can be selected to reach the nasal cortex if the anatomy allows it.
Case Studies About The Nasal Floor Cortex
-
Failed All-on-6 Saved with Basal Implants
Dr Genchev saved Françoise after she suffered a failed All-on-6 procedure. Full dental restoration with basal dental implants in 5 days treating prognathism for €9,990.
-
Dental restoration for missing teeth and bone atrophy with basal implants
Dr Genchev completed the full mouth dental restoration for this patient who suffered from edentulism with severe bone atrophy in 1 visit of 5 days. The price for the full dental restoration was 8990 Euro.
